Monkeypox
Emerging Diseases

Welcome to Science with Shrike! Today we cover an emerging disease that has been progressing through the US and other countries that do not normally find it: monkeypox. Is this COVID round 2?
Monkeypox spread
So what about monkeypox? Of the infection routes described in the last post, monkeypox is spread via mucosal contact. Infectious material that comes in contact with either tiny breaks in your skin, or mucous membranes (including the anus, or mouth) can start the infection. These are primarily respiratory droplets and contact with lesions, but also contact with environmental samples contaminated with infectious material (aka fomites). So avoiding contact with the infectious material being shed by infected people is the main goal of mitigation. Monkeypox is sensitive to UV irradiation, as well as the usual disinfectants (eg bleach), so areas can be decontaminated as needed. The smallpox vaccines also work against monkeypox, though we are about to get clinical data in how long cross-protection lasts.
Monkeypox takes 5-24 days (average 12 days) for symptoms to appear. This starts as feeling sick (eg fever, sweats, muscle aches headache) and outbreak of lesions. These lesions are not limited to the site of infection, but in the gay community, most of the lesions have been in the anal, perineal or genital regions, which lends it to spread as a sexually transmitted disease. To see what this does to your genitals, check out this BMJ article. Penile edema and the pain are no fun, even if the fatality rate for monkeypox is low (12 deaths reported out of 31,799 cases world-wide, as of Aug 10). If you think ‘not fatal’ is no big deal, check out the article. Scroll to the end for the pictures.
US cases are increasing exponentially, and monkeypox has spread to many nations that do not normally see monkeypox. Looking at the US cases, we see exponential spread.
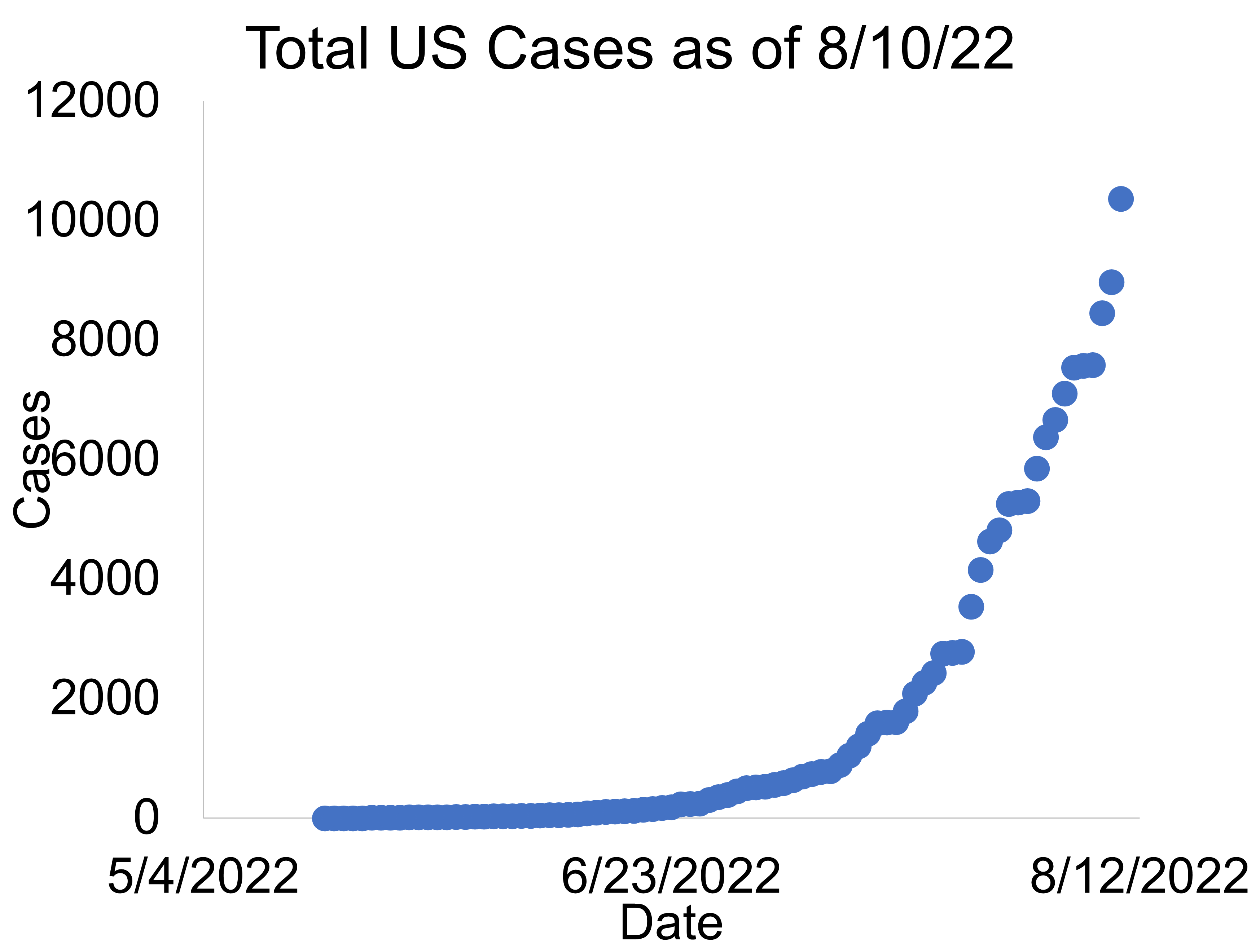
In fact, after the initial spike in cases (potentially an anomaly of poor reporting), the growth has been perfect, constant exponential growth. This suggests the disease is spreading rapidly, with no changes to spread. On one hand, this could mean that any public health level interventions have had no effects so far, and the disease has not jumped into new populations and/or become more infectious. The alternative hypothesis is that benefits from public health interventions are perfectly outweighed by new infectivity. Since the disease has a 5-24 day incubation period, there will be a lag of 2-4 weeks between what the numbers reflect any changes made today.
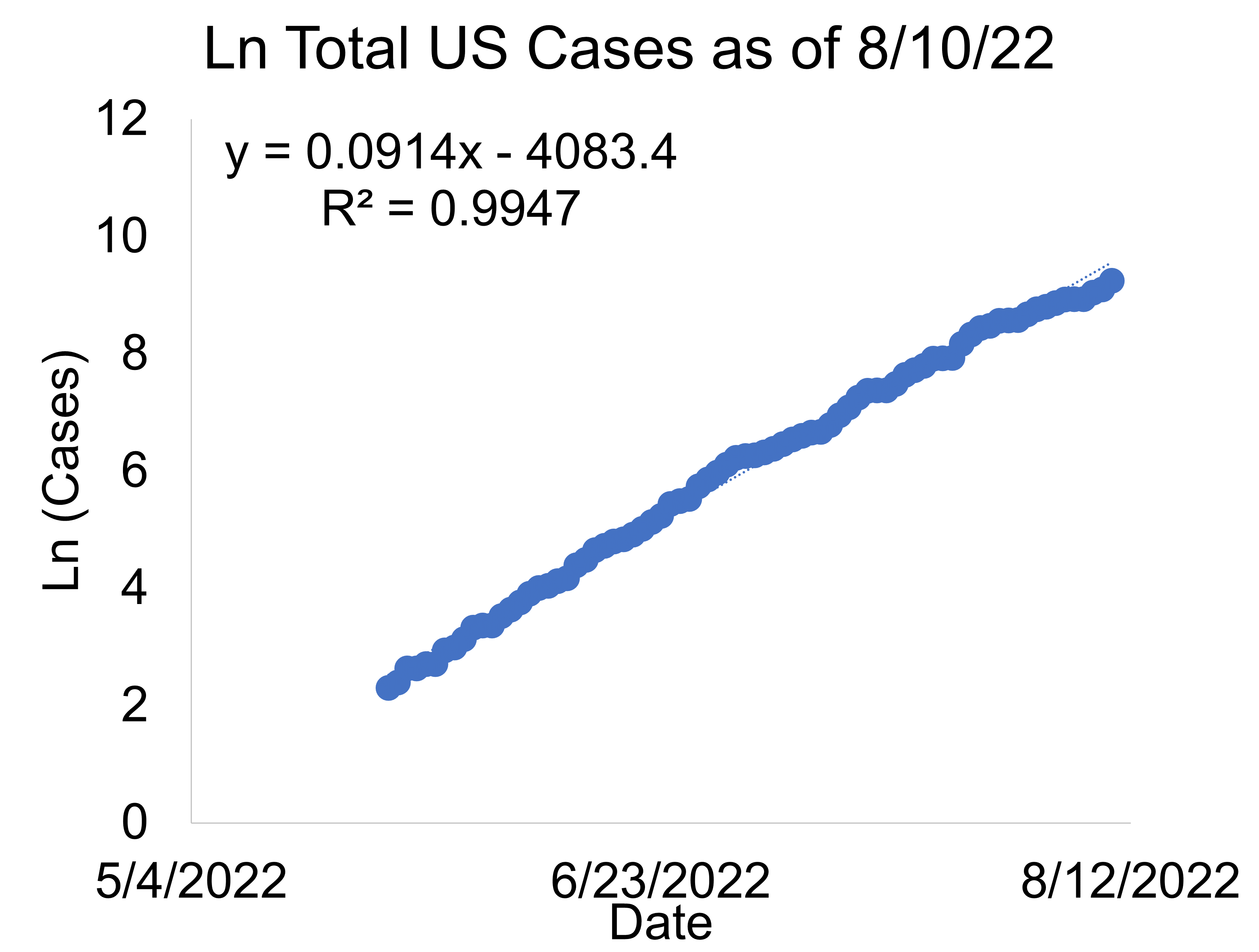
One interesting note is that the number of monkeypox cases has been doubling every 8 days. If the ’12 day average’ to new symptoms is accurate, this would imply an R0 of 2. Recall R0 is the rate of spread (the average number of new infections per infection). Smallpox historically had a maximal R0 of 3, so this rate of spread is not unusual for a pox virus. Note that measles has a maximal R0 of 18 and polio 5. Keep in mind these are back-of-the-envelope numbers based on estimates, so these should be considered ballpark numbers, not precise answers, and that R0 changes as conditions change (ie decrease in susceptible population).
If you want to project case growth, type the date into excel, and then convert it to a number. That number goes into the equation on the chart in place of the x and will give you y. Once you get y, you need to raise e to that power. In excel, just use =EXP(y) For example, if the case growth remains constant, by Christmas 2022, there will be 4.7 billion people in the US infected. This is a reminder that you need to be careful with predictive modeling. There aren’t 4.7 billion people in the US, so this level of exponential growth will taper. It also means that if there is some new change in the disease that accelerates infection, this pandemic may be over even faster (at current rates, everyone in the US gets infected by Nov 26, which is 2 days after Thanksgiving). However, it is important to emphasize that the current infection rates are not sustainable even if we change nothing. As the susceptible population density decreases, the infection rate will also drop.
When it will taper, and whether that taper will have anything to do with any public health responses vs decrease in susceptible population, are the big questions. Part of this depends on what scenarios you think will play out. Shrike will outline a few different scenarios for how this could play out.
Scenario 1 Limited disease. In the best of all worlds, monkeypox remains limited to the gay community, and there is negligible transmission outside of men having sex with men. A random internet source estimates that there are ~13M LGBT people in the US (~3.8%). Let’s assume half are gay or bi men, and half of those are promiscuous. This would give us a susceptible population of 3.25M. As of Aug 10, there are ~10k cases in the US, so ~0.3% of the susceptible population is infected. With no changes, Sept 23 is when we hit 1M cases at current rates, which would give ~30% infected. Rate would likely taper at some point around there, so it would then be a slow crawl up to ~3.25M, at which point the disease dies out.
This is a back of the envelope calculation using numbers that are essentially made-up, so if you put more accurate numbers in, you will get more accurate results. For example, maybe only 10% are promiscuous. Maybe gay men represent less than half of the LGBT population. Maybe the population estimate is wrong. Note that shrinking the susceptible population means it tapers sooner, larger population means it tapers later.
Main take-away is that in this scenario, monkeypox will look like cause for panic running through September and suddenly cease to be an issue in October or November because case rates may start dropping. This coincides with the US midterm elections, so cynical people may assume that public health officials are manipulating the disease to win votes for their party. However, please note that the math did not account for public health responses—Shrike’s prediction is that if it stays limited to the promiscuous gay community, it will taper in the next few months.
Scenario 2 Widespread sexually transmitted disease. Since there are promiscuous people who have sex with both men and women, there is no a priori reason why this cannot spread to promiscuous people outside of the gay male community. In this scenario, monkeypox becomes one more STD like herpes, chlamydia or gonorrhea. Cases would be predicted to increase faster in more promiscuous countries compared to less promiscuous ones once it gets into the general population. It’s challenging to predict when disease would peak in this scenario, because it is challenging to estimate the total number of people who would be susceptible. If we assume that 235M people are over 18 in the US, and 10% of those are promiscuous, that’s 23.5M susceptible people. We hit 30% of that population on October 27 at current rates. Rates will start to taper around the midterms in this scenario. However. Shrike would expect the disease to become endemic. It will be added to the list of STDs you can catch.
Scenario 3 Widespread disease. Since monkeypox is a mucosal infection, it may not remain a sexually transmitted disease. It may be passed to roommates or family members. Also, people don’t wash their hands after using the bathroom, let alone other activities, so it may be spread through poor hygiene as well. Once it gets into little kids, it will continue to spread because little kids spread diseases very well between each other and their parents. Since rodents and other animals can also be infected, it is possible one or more animal reservoirs are established. One risk in this scenario is that children under 8 have more severe disease, so day cares may run into serious problems. Another risk is that the presence of animal reservoirs will complicate eradication efforts.
Since monkeypox is NOT spread as well as respiratory infections, spread is slower and easier to contain. Shrike expects that in this scenario, the disease slows the rate of spread once it gets into the general population because it is harder to transmit at a daycare of 10 vs an orgy with 30 sexual partners. However, while the disease may slow somewhat, it will not taper the same way as it would in a limited population—it’ll just switch to a slower grind up. In this scenario, expect an over-zealous public health response. When that response comes will depend on the politics.
Shrike thinks Scenario 3 is how monkeypox will play out—it will move into the general population (best monitored by infection rates in children), and then spread more slowly through the population due to poorer transmission, individual responses, and public health measures.
Individual Health Measures
After fear of ‘what will monkeypox do to me and my loved ones’, many people jump to two questions: ‘what should I do?’ and ‘what should the public health response be?’. We’ll cover the individual options first and then the public health options based on the scenarios outlined above.
When it comes to treatment, prevention is the best strategy. Your prevention options are to reduce your potential exposure to monkeypox, or to build immunity via vaccination. Your current vaccination options are smallpox vaccines. There are two smallpox vaccines: ACAM2000 and JYNNEOS. ACAM2000 is live Vaccinia virus, which replicates and causes an infectious lesion. After 28 days, you are vaccinated. JYNNEOS is a non-replicating live virus given as two shots 4 weeks apart, it does not cause an infectious lesion, and you are considered vaccinated 2 weeks after the last shot.
The smallpox vaccines provide protection against monkeypox, with evidence from prior African outbreaks suggesting ACAM2000 has ~85% efficacy. JYNNEOS efficacy is assumed based on success in preclinical trials, and its cross-reactivity with monkeypox. There are no vaccine efficacy data yet for either vaccine in humans from the current outbreak.
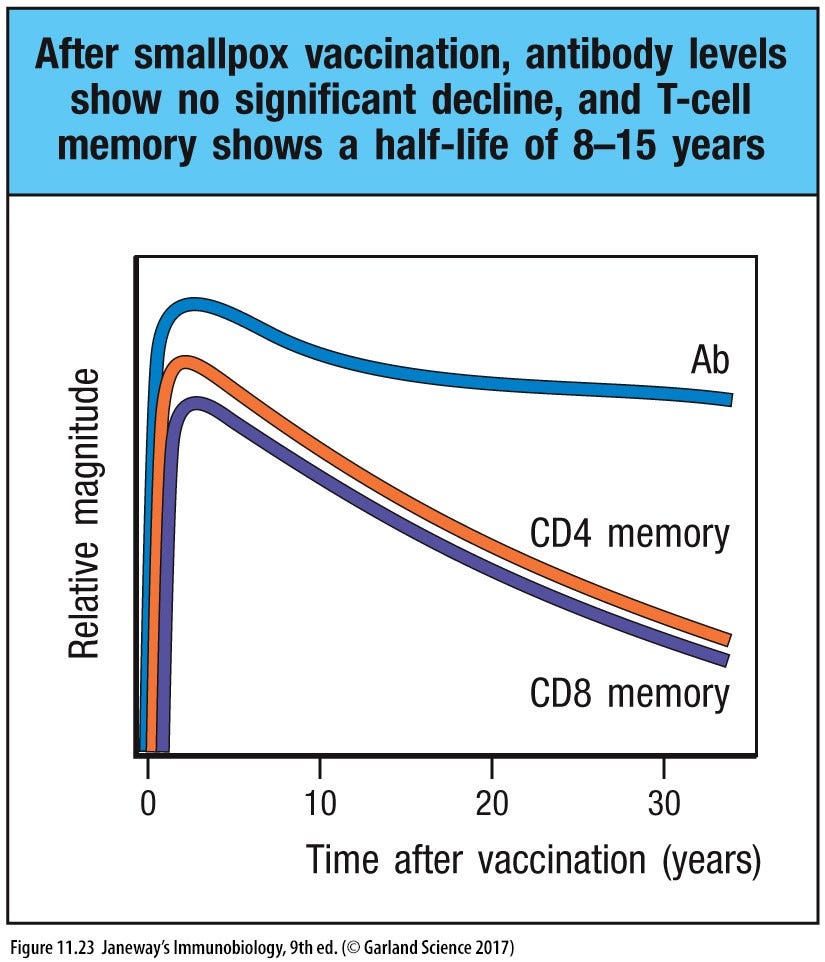
Whether the smallpox vaccination you (or your parents/grandparents) received 50 years ago still protects is an open question. Antibody titers do not decline much over time, but T cell memory responses to smallpox have a half-life of about 8-15 years. This is why the current recommendation is to get vaccinated again if it’s been more than 3 years and you are exposed to monkeypox.
While ACAM2000 contains an attenuated virus, if you are immunocompromised, it can cause serious problems for you. With JYNNEOS, this is expected to be less of a problem because the virus does not typically replicate. With ACAM2000, there is the potential to transfer the virus to other people. Shrike observes that if you were to attempt to transfer Vaccinia to a willing recipient, they will also risk exposure to any other bloodborne pathogens you have. In addition to any liability from the transfer going wrong, it may also be illegal in your jurisdiction. Consequently, Shrike recommends AGAINST this approach.
ACAM2000 carries more side effects than JYNNEOS because it is a replicating virus vs a non-replicating virus. However, there is a small (Shrike estimates ~1 in a million to one in a trillion, depending on how JYNNEOS is manufactured) chance that a replicating Vaccinia virus is made with the JYNNEOS vaccine. In this case, it would be expected to behave more like the ACAM2000 vaccine. Both vaccines rely on cross-reactivity between pox viruses to provide protection against monkeypox. JYNNEOS is FDA-approved for both smallpox and monkeypox, whereas ACAM2000 is approved for smallpox, but has an emergency use authorization for monkeypox. Neither are approved for kids under 18.
The vaccines can be given in two scenarios: pre-exposure prophylaxis (what you normally think of as a vaccine), and post-exposure prophylaxis. Currently pre-exposure prophylaxis in the US is limited to research personnel working on pox viruses, clinical personnel involved in testing monkeypox, administering ACAM2000, interacting with patients with monkeypox, and specific designees of public health authorities. If you can volunteer for a lab working on Vaccinia or one of these other efforts, you may be able to get vaccinated. Shrike suspects the limitations on who can get vaccinated are due to limited vaccine availability, and limited vaccine data.
Post-exposure prophylaxis is available to those with known exposure to monkeypox. When received within 4 days of exposure, it is hoped that it prevents disease onset. After 4 days post-exposure, the hope is that it reduces disease symptoms. Maybe post-exposure prophylaxis will work, but the data are not yet available. Depending on efficacy in this modality, it might reduce the pre-exposure vaccine course as well.
Since the vaccines take 4-6 weeks to provide protection, if you think you will be at risk, and want to get vaccinated, it is best to get vaccinated in advance of when you think you will need it. If you are not at risk, it does not make sense to vaccinate at this time.
Scenario-specific Individual Prevention
In scenarios 1 and 2, the individual response is simple. Avoid promiscuous sex. If people you live with have promiscuous sex, you might consider taking some of the precautions laid out for scenario 3. If you choose to have promiscuous sex anyways, take the same precautions that you would for gonorrhea, herpes and other STDs. Use condoms, avoid contact with any obvious lesions, regular testing.
If you have an active infection, wait for the infection to resolve. Covering lesions with band-aids for intimate contact might help a little, but well, it’s … a band-aid solution. Do you really care so little about your sexual partners that you want to give them something like this? Just wait for the infection to resolve.
{kind=link}
Scenario 3 becomes more challenging. The good news is that infection requires contact with infected material from the lesions, or possibly respiratory droplets. The lesions are often obvious, and respiratory droplets (in contrast to aerosols) can be blocked by masks. It is unknown if monkeypox is transmitted asymptomatically or via other bodily fluids (feces, urine, saliva, snot, semen), though if any of those are mixed with blood, the fluid is always considered infectious. There are not yet any reports of transmission by proximity, which suggests respiratory routes may not be large drivers of infection.
Make a plan
Plan for both dealing with the public and dealing with family and roommates. When dealing with family and roommates, communicate with them. If you have trouble communicating with them, it’s time to either move out or fix the communication issue. Not because of monkeypox, but because you need to effectively communicate with anyone living with you. This way you can develop a household plan for dealing with infections, including monkeypox.
A plan is expected to save your household pain and consternation in the long-term. For adult roommates, you establish clear boundaries and expectations. If planned in advance, you are able to discuss disagreements without it being as personal. For children, a plan will help both you and them weather the pandemic because they will have clear expectations about what to do, and they know what they need to do to be prepared. A plan is expected to reduce anxiety because there is less uncertainty surrounding what happens next, and they know mommy or daddy can’t touch them because of the lesions. Even if an infection happens, you are prepared to handle it.
The CDC has extensive recommendations for reducing your risk, caring for those with monkeypox, caring for pets, dealing with active infections, and decontaminating fomites. Overall, the current recommendations are reasonable. Expect that they will change as we learn more about this pandemic—these guidelines are based on prior monkeypox outbreaks and expertise.
The tl;dr version:
Prevention
Avoid close contact with lesions and people who have them, avoid linens/clothing from people with monkeypox, and wash your hands. Don’t have random sex with strangers.
Caring for infected individuals
Gloves for all potential infectious contact. Avoid lesions. Take care with linens/clothing and launder them. Decontaminate areas regularly.
Pets
Treat them like people—don’t expose them, don’t abandon/kill them if they are exposed, don’t soak them in any disinfectant you wouldn’t soak your kid in, and monitor for symptoms.
Active infection
Isolate if possible, cover lesions and avoid close contact with people and pets if not, decontaminate surfaces you use, deep clean once infection resolved.
Decontaminate fomites
Be careful with laundry and other linens. Think about commercial services where linens might be shared or re-used (spa, AirBnB, etc). Have infected people do their own laundry when practical. Decontaminate environment w/EPA-registered disinfectant (eg dilute bleach to 10% fresh each time, or use bleach wipes). Soft surfaces (carpet, cloth-backed chairs) can hold virus better than hard surfaces, and they’re harder to decontaminate. Try to avoid aerosolizing any particles (dry sweeping, shaking potentially infected linens out, etc) when cleaning.
Public Health Responses
What public health measures will help fight monkeypox? Before we discuss potential options, let’s consider the goals of any proposed public health policy. Shrike believes the goals of the public health response to monkeypox in all 3 scenarios must accomplish 5 key targets:
Reduce monkeypox transmission
Reduce hospitalizations and deaths due to monkeypox
Eradicate monkeypox infections in the US
Minimize other negative health impacts from public health interventions
Do not overthrow the historical, core governing principles of the US
Reduce transmission
Goal #1 is to cut the transmission down. The exponential growth suggests no public health interventions have worked to curb transmission so far. Breaking transmission is best achieved by decreasing the density of susceptible people—this means immunity either via infection or vaccination. It also needs to be monitored and public health messaging put out.
Vaccines
We already have a vaccine that worked for prior monkeypox outbreaks—ACAM2000. Ramping up production and distribution are logistic challenges. Even in scenario 1, there is a susceptible population of ~3.25M, plus all of the healthcare workers and other providers associated with administering to that population. Distribution needs to be prepared to handle the demand. Once supply is in place, the vaccine should be available to any who want it.
Adding additional vaccine capacity and data are also important. JYNNEOS has the potential to be a better vaccine, so we need to get human, clinical data on that one to ensure it lives up to its promise. With neither vaccine approved for children under 18, we need to start trials now to test their safety in them. Imvanex is another vaccine that was used in a 2018 monkeypox outbreak in the UK.
Validating the vaccines for cats and dogs would also be important to help prevent any establishment of monkeypox in those mammals and to give people an option to protect their pets.
One challenge for testing new vaccines is identifying the at-risk population. If you need to vaccinate 40,000 people for enough people in your treatment arm to be exposed to monkeypox, this is an expensive and logistic challenge in its own right.
At the public health level, these goals are accomplished in part by pre-purchase of vaccines, funding clinical trials, and removing red tape from approval and trial design processes. Public health authorities can also help by connecting at-risk people with clinical trials so they can get the prophylaxis they need.
Surveillance
Improved surveillance is another key feature of reducing transmission. This requires testing contacts and high risk people. This is another logistic and distribution challenge, along with adding a reporting challenge.
One challenge with testing is getting the right amount of testing. Since monkeypox is not routinely spread via aerosols, an obsession with testing everyone wastes money and desensitizes the public to public health messaging and testing. Testing should be focused on those with potential exposure or engaged in high risk activities, and NOT on ‘you need a negative test in order to fly’.
Given the risk-averse nature of companies and other institutions, they will adopt whatever the government recommends to limit their liability risk. The public health response needs to provide protection to the people served by these companies and institutions. Consequently, explicit statements about testing (that can be challenged by the public) should be developed, either on a conditional (these are the circumstances in which we recommend a test) or other basis.
Messaging
The other tool public health authorities have is the messaging put out to everyone. This kind of messaging needs to be simple, focus on the majority, and leave some room for the inevitable exceptions. For example, ‘don’t attend orgies right now’ would be an excellent message at this stage. Other hygiene and prevention messaging may also be helpful, but the message needs to stay focused.
While one temptation with messaging is to become authoritarian (‘do this or else’), the messaging is more effective when done persuasively, and when partnered with other stake-holders. Since monkeypox predominantly affects promiscuous gay and bi men right now, working with gay rights groups, and influencers popular in the gay community to spread the message will be more effective than tepidly posting ‘avoid sexual contact with infected people’. As the pandemic progresses to scenarios 2 or 3, engage people active in those communities to help frame the message and get it out to people.
Another temptation is fear mongering. This is a hard balance to strike. On one hand, fear sells, so scaring people is a legit marketing tactic to move them to action. On the other hand, too much fear costs credibility, and may lead the public to demanding restrictions from their government to ‘feel safe’. It may also be challenging to unwind all the fear once the pandemic ceases.
Reduce hospitalizations and death
While reducing transmission is linked to reducing severe disease, dealing with severe disease remains a challenge. Tecovirimat is one drug in trials that might be useful to this end. Currently, more data are needed to formulate specific plans to reduce severe events beyond ‘avoid infection’.
At first, this is best informed by case studies (eg physicians trying different approaches based on their experience) and then promising approaches tested via clinical trials. Developing entirely new antivirals is a long-shot, as monkeypox is either endemic or over by the time they would see market.
Also expect to see many home cures, “detox”, and other remedies pushed by twitter as cases ramp up. Shrike would remain skeptical of anecdotal evidence until it is rigorously tested. However, Shrike would like to see promising leads tested instead of decried by the media. If the home remedy does not carry significant toxicity, public health authorities waste their time, energy, and credibility challenging most of these. Instead, the messaging is more effective if public health officials stay on their message, recognize that most people enamored with a particular treatment want people to benefit, and hold all leads to the same standards of evidence.
The other angle that can help reduce hospitalizations and death is reducing comorbidities. Explicit messaging on this topic was ignored for COVID-19 to great detriment, but this should not be missed for other pandemics. It serves two purposes: 1) gives people something physical to do, so they feel like they are helping with the effort and 2) reduces healthcare burdens, freeing up resources to deal with new pandemics.
Eradicate monkeypox infections in the US
While success with the prior two goals may accomplish this one, eradication needs to be explicit. As of Aug 10, ~10k cases are present in the US, so this disease can be stopped in its tracks with aggressive early action (i.e. solve logistics on vaccine production and surveillance, message at-risk populations)
In scenarios 2 and 3, monkeypox may become too widespread to handle via messaging and self-isolation, and ends up being endemic. To ensure eradication, a vaccination program will be the most feasible route to accomplish this goal. Given the low death rate, and expected lower spread, this does not need to be rushed. If the disease is endemic, there will be enough patients for testing, and voluntary vaccination is expected to be sufficient over a 2-3 year period.
If not, addition of the smallpox vaccines to the regular vaccine course should be considered, but only after extended comments from the public, human clinical trial data with this outbreak are available, and the disease becomes endemic in the susceptible population.
Minimize other negative health impacts from public health interventions
When evaluating approaches to accomplishing the former 3 goals, they cannot be considered in isolation. The consequences of any public health interventions needs to be considered and the costs weighed vs the benefits achieved. Benefits need to be validated before they are used to roll out a national program. For example, the JYNNEOS vaccine needs more testing before it should be touted as the best solution to the monkeypox pandemic.
Another example is that universal masking does NOT carry enough benefits to warrant that implementation. Individuals may decide to mask based on their risk estimates, but at the public health level, controlled trials are needed to show a benefit before implementation.
Visitation bans in hospitals would similarly need to be carefully weighed against the harms they might cause, and be limited to cases where the benefits are clear.
Shutting down daycares and/or schools might be considered if it spreads in children. However, data are needed to support either choice, given the clear costs these measures have. While Shrike expects daycares to be germ centers, that suspicion is insufficient grounds on which to base public health policy. Data are needed, and even then, people may be able to make their own decisions on the risk to their children.
This is a fine line to walk, and will end up a judgment call, depending on your biases and beliefs. To that end, this goal needs to be discussed in public, along with all other considerations from multiple stakeholders. For example, current US responses have tried to balance anti-monkeypox messaging with other concerns. For example, health officials have been reluctant to point out monkeypox is currently spread primarily between gay men. Echoes of the start of the HIV pandemic have led to a fear that by focusing on gay orgies, the gay community would be stigmatized, and the risk to everyone else minimized. The strength of this response is that it is considering other aspects of policy when choosing monkeypox messaging. The weakness of this response is that there are no data suggesting the gay community is being stigmatized over monkeypox, nor that the community would be put at increased risk by saying ‘hold off on the orgies for now’. Conflating the entire gay community with massive orgies in the minds of the population is also a weakness of this reluctance.
Do not overthrow the historical, core governing principles of the US
There is a strong temptation with public health to become authoritarian. Legislative bodies are slow, and executive (or even public health level) decisions are much faster. People will inevitably make suboptimal decisions, and these decisions may either put others directly at risk, or cost health care resources. Making decisions for them seems like it is easier for all parties.
Aside from being associated with the largest bioterror attack in the US, Osho also made key insights into democracy that many agree with, even if they might say it differently.
Ordering people around can accomplish specific policy goals. In some cases, that might even be necessary. However. Those cases are the exception rather than the rule.
For example, closing businesses like spas over monkeypox would fall into the ‘overthrowing core governing principles’. Vaccine mandates for monkeypox in order to exist in society would also fall into this category. Suppression of “misinformation” also fits here because “misinformation” means ‘everything with which the regime disagrees’. Free and vigorous discussion are both a foundation of the US, and beneficial to improving public policy.
If you have a public health official pushing for government over-reach, the best thing that can be done for public health is to publicly fire them and distance yourself from them. Trust is low in public health due to the public health abuses during COVID-19. That trust needs to be restored, and that comes from including the public in discussions, resolving objections, and working from the most up-to-date, publicly available data.
Without trust, the only option left to public health is authoritarian rule. This becomes a death spiral because a subset of people will resist authoritarian rule simply because it is authoritarian rule. This leads to police crackdowns, which angers more people, and proceeds to fracture society.